Our Technology
MAKO robotic assisted joint replacement is an exciting new development in joint replacement surgery which allows surgeons to plan according to the patient's SPECIFIC anatomy.
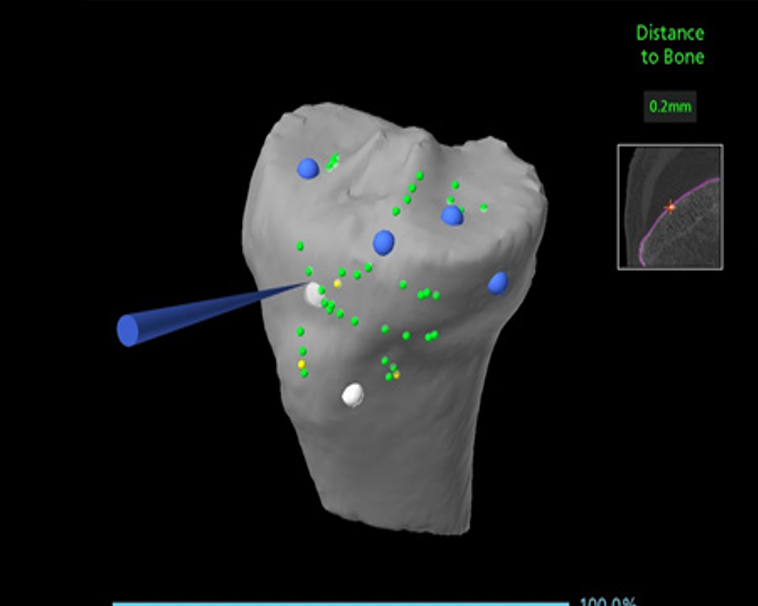
This is based on a CT scan of the knee joint with computer software used to create a digital image of your knee. This is then fed into the Mako Robot where a 3D image is created.The surgery is then planned with meticulous detail with more accuracy in terms of angles, size of the implant and positioning of implants to get appropriate soft tissue balance to suit your anatomy and to restore, as far as possible, any changes created by the arthritic changes.
This is almost a virtual trial run of the surgery about a week or so prior to actual surgery and makes sure that surprises at the time of surgery are kept to a minimum. It helps to fine tune position of implants to obtain optimum soft tissue tension prior to actually making the first incision.
The robot does not perform the surgery. It only helps the surgeon in the planning and performing of the replacement. For this some sensors need to be placed in the thigh bone and the leg bone temporarily. There is a theoretical risk that this can cause the bone to weaken and break if repeated attempts are made to place the pins. These pins will be removed once the surgery is completed.
SHOULDER REPLACEMENT SURGERY
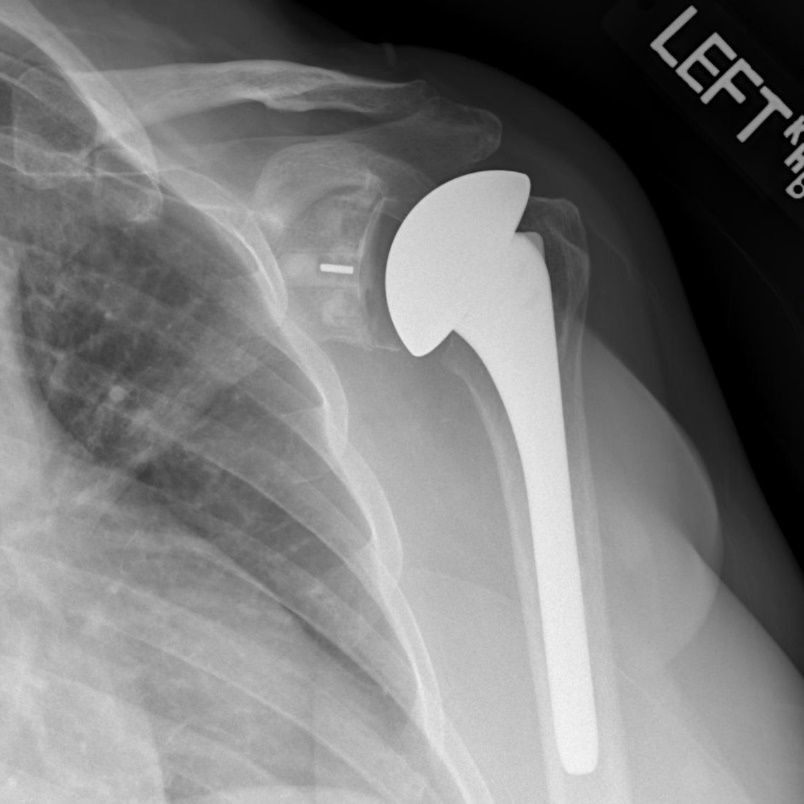
Shoulder replacement surgery is indicated for painful, stiff, arthritic shoulders or sometimes in fractures when it is difficult to reconstruct with plates and screws. In some patients with irreparable rotator cuff tears, we may have to resort to a shoulder replacement
(1)Anatomic (“normal”) shoulder replacement means replacement of like with like; we replace the socket with a new socket and the ball joint with a new ball on a metal stem. . For this to be successful, a basic requirement is that normal tendons are present in the shoulder to maintain a fulcrum for the joint to move normally. If tendons are weak or become weak later due to ageing, the shoulder cannot move normally and tends to slide upwards.
(2) Reverse Shoulder replacement
If the tendons of the rotator cuff are badly torn or unhealthy and cannot be repaired, an anatomical replacement will not work properly as there is no stable fulcrum. In such a situation we resort to a Revese shoulder replacement. In a Reverse shoulder replacement, the socket is replaced with a ball prosthesis fixed to the shoulder blade and the socket is fixed to a metal stem inserted into the humerus bone. This is done in order to maintain a fulcrum for the shoulder to move when the tendons are torn off or weak.


(3) CTA Hemiarthroplasty
In some patients the bone in the socket is too thin or soft and either the metal implant cannot be safely impacted into the bone or the metal implant gradually loses position if the bone support is not enough. In such cases an alternative option is to replace only the ball part of the joint with a flanged implant which offers additional support to the joint to maintain movement.
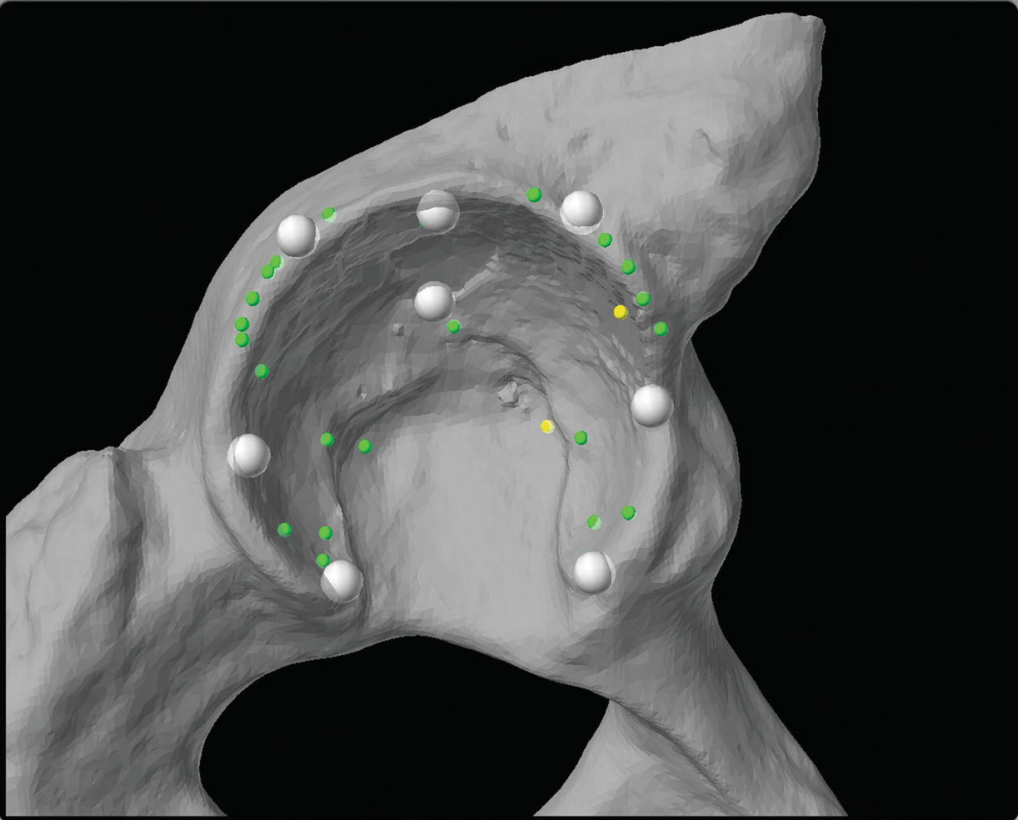
Dr. Rajesh uses Patient Specific Guides for precise implantation of the artificial socket. CT scan of the shoulder is taken and a 3D model is developed from this. On a virtual platform the position,orientation and size of the implant is planned.
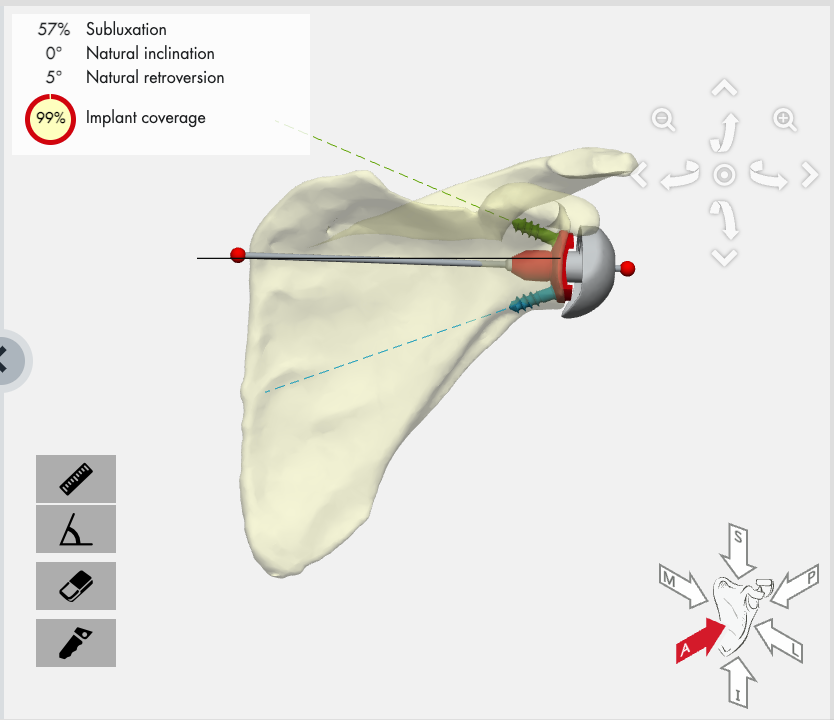

The planned position is achieved during surgery by using Patient Specific guides based on the particular patient’s anatomy. These guides are sterilised for use in surgery and fit perfectly to the socket allowing guide pins to be inserted accurately. The guide pins allow the drills and reamers to create a slot for the implant to go into as planned on the CT scan.
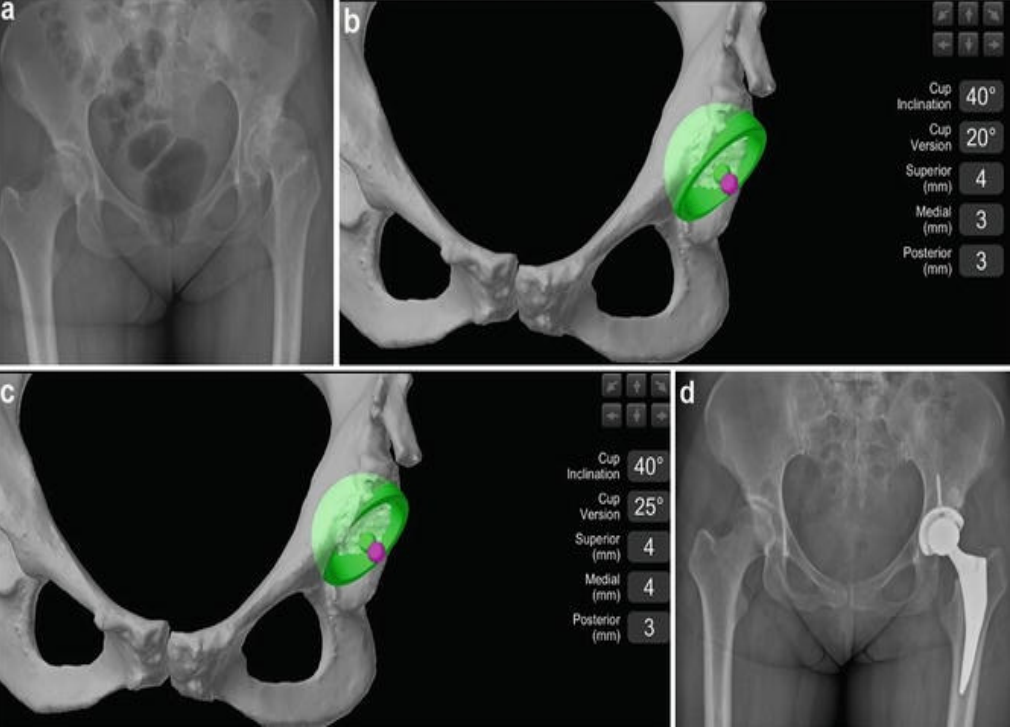
MAKO robotic assisted joint replacement is an exciting new development in joint replacement surgery which allows surgeons to plan according to the patient's SPECIFIC anatomy. This is based on a CT scan of the hip joint with computer software used to create a digital image of your hip. This is then fed into the Mako Robot where a 3D image is created. The surgery is then planned with meticulous detail with respect to the size of the socket (Acetabular component) to be used, the ideal angle of inclination and version of the implant to suit your anatomy and to restore, as far as possible, any shortening or angulation created by the arthritic changes.
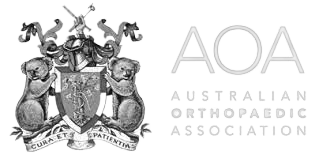
The model generated by the robot using the CT scan is then matched to the actual patient anatomy by precise mapping of multiple bony landmarks in the patient.This allows the Robot to "see" where the surgeon is placing the reamer to prepare the bony socket and also how and where the new socket is being implanted.Thus very precise control of the socket preparation and implant positioning can be facilitated by the robot.The robot DOES NOT perform the surgery.